






Innovation or Evergreening?
A Practitioner’s Detailed Analytical Guide
Covering Malaysia · Indonesia · Thailand · Philippines
By Phylicia Yeoh
The Question That Divides an Industry
Every patent attorney working in the pharmaceutical space has encountered the same uncomfortable question: When does legitimate innovation end and strategic maneuvering begin? Nowhere is this tension more vivid or more consequential than in the doctrine of secondary pharmaceutical patents.
A secondary patent does not protect a new molecule. It protects something further downstream: a new salt form, a new polymorph, a new therapeutic use, a new formulation or dosage strength. In theory, such improvements can transform a medicine, making it more bioavailable, more stable on the shelf, safer to administer. In practice, the same legal instrument has been documented as a tool for extending market exclusivity well beyond the original invention, a phenomenon critics call “evergreening.”
"Patent systems are not just about incentivizing innovation. They are about structuring the social contract between inventors and the public and that contract has terms."
— Peter Drahos, Intellectual Property and Public Health (2008)
This question carries enormous stakes in Southeast Asia (also known as ASEAN). With a combined population exceeding 680 million people, a rapidly growing middle class demanding higher-quality healthcare, and domestic pharmaceutical industries seeking competitive parity, the region’s legal frameworks governing secondary patents are not merely technical curiosities. They are instruments of public health policy, economic strategy, and innovation governance, simultaneously.
KASS International has advised pharmaceutical innovators and generic manufacturers across Malaysia, Indonesia, Thailand, and the Philippines for more than two decades. What follows is our practitioner’s guide to the divergent secondary patent landscapes across these four specific jurisdictions filtered through the insights of the world’s leading IP and pharmaceutical patent scholars.
Part I: The Intellectual Framework: Five Thinkers Who Shape the Debate
1. Peter Drahos: Patent Systems as Social Contracts
Australian National University professor Peter Drahos has spent his career interrogating the political economy of intellectual property. His landmark work, co-authored with John Braithwaite, Information Feudalism (2002), exposed how pharmaceutical companies leveraged international trade mechanisms (particularly TRIPS) to create a global IP system that served their interests at the expense of developing nations.
For Drahos, the critical analytical question is not whether a secondary invention is technically novel, but whether granting a patent for it serves the social contract that justifies the patent system in the first place. He argues that patent offices in developing economies, which lack the institutional capacity to conduct rigorous prior-art searches and inventive-step analyses, are particularly vulnerable to granting low-quality secondary patents that hollow out the public benefit of the system.
Drahos Lens: Practitioner Application
When advising on secondary patent prosecution in Southeast Asia, ask not only whether the claim meets the formal patentability requirements, but whether the improvement being claimed delivers genuine public benefit. Patent offices that apply Drahos’s framework, like the Philippines, will ask exactly this question and will expect a compelling answer.
2. Carlos Correa: The Anti-Evergreening Architect
No single scholar has influenced pharmaceutical patent policy in developing nations more directly than Carlos Correa of the University of Buenos Aires and the South Centre. His 2006 Guidelines for the Examination of Pharmaceutical Patents: Developing a Public Health Perspective, prepared for the WHO, UNCTAD, ICTSD, and the World Bank became the intellectual blueprint for what is now known as “Section 3(d)-style” anti-evergreening provisions, following their adoption in India.
Correa’s central argument is elegant: The standard of inventive step as applied in most national patent offices is insufficiently demanding for pharmaceutical secondary patents, because the relevant comparison is not whether a skilled chemist could have predicted the modification, but whether the modification delivers a clinically meaningful therapeutic advance. His framework directly informs the Philippines’ enhanced therapeutic efficacy requirement, arguably the strictest in ASEAN.
"The grant of secondary pharmaceutical patents without requiring evidence of enhanced therapeutic efficacy can serve no purpose other than extending monopoly rights."
— Carlos Correa, Guidelines for the Examination of Pharmaceutical Patents (2006)
Correa also pioneered detailed analysis of the specific subject-matter categories that are most commonly used for evergreening: polymorphs, salts, esters, hydrates, ethers, metabolites, particle-size modifications, and prodrugs. His taxonomy remains the definitive practitioner reference for understanding which claim types will face heightened scrutiny in anti-evergreening jurisdictions.
3. Jerome Reichman: The Flexibility Architect
Duke University’s Jerome Reichman occupies a different position in this debate. While sympathetic to public health concerns, Reichman’s most influential contribution has been his rigorous articulation of the TRIPS flexibilities available to developing nations and his critique of over-restrictive domestic patent laws that, paradoxically, can harm local innovation ecosystems.
Reichman’s work on “calibrated exceptions” argues that developing nations are entitled under TRIPS to design patent laws that serve their specific development stage, industrial capacity, and public health priorities including broader Bolar exemptions, compulsory licensing provisions, and flexible approaches to patent term. His framework is particularly visible in Indonesia’s 2024 reforms, which simultaneously expanded secondary patent protection (serving pharmaceutical innovators) while strengthening Bolar exemptions and parallel import rules (serving generic manufacturers and patients).
Reichman Lens: The Indonesia Paradox
Indonesia’s Law No. 65 of 2024 is arguably the most sophisticated example of Reichman-style “calibrated flexibilities” in ASEAN: it expands the scope of protectable inventions while simultaneously strengthening the public health safeguards that limit the practical effect of that expansion. Understanding this dual architecture is essential for advising clients on post-2024 Indonesian pharmaceutical patent strategy.
4. Dan Burk and Mark Lemley: The Patent System's Policy Levers
Stanford’s Mark Lemley and University of Minnesota’s Dan Burk, in their seminal article The Patent System for the 21st Century (2003) and subsequent book-length treatment, introduced the concept of “policy levers”, the idea that the same doctrines (obviousness, written description, claim construction) can and should be applied differently across different technology sectors because the economics of innovation differ radically between industries.
Their insight is directly applicable to pharmaceutical secondary patents. They observe that the pharmaceutical sector is unique in the patent landscape: it is the industry where the patent system is most essential to recouping R&D investment, but also the one where patent claims are most readily subject to incremental extension strategies. The appropriate policy response, they argue, is not to weaken patent protection generally, but to calibrate the application of patentability standards, particularly inventive step and industrial applicability to the specific economic realities of pharmaceutical R&D.
This framework helps explain why Malaysia’s general patentability approach, while defensible, leaves pharmaceutical innovators in an environment of strategic uncertainty: without pharmaceutical-specific guidance, both innovators and generic manufacturers face unpredictable outcomes in prosecution and opposition proceedings.
5. Amy Kapczynski: Access, Innovation, and the Knowledge Economy
Yale Law School’s Amy Kapczynski represents a newer generation of IP scholars who situate the secondary patent debate within the broader political economy of knowledge production. Her work on the “access to knowledge” movement and on pharmaceutical patent evergreening in the United States, particularly her contributions to the landmark study of secondary pharmaceutical patents in the U.S. market offers ASEAN practitioners a crucial analytical tool: empirical evidence.
Kapczynski’s research demonstrates that secondary pharmaceutical patenting is not a marginal phenomenon. Her work shows that the most commercially successful drugs attract the most secondary patents, and that these patents correlate strongly with delayed generic entry. For ASEAN practitioners, this empirical grounding is important: it confirms that the policy concerns driving countries like the Philippines toward strict anti-evergreening rules are grounded in documented pharmaceutical industry behavior, not theoretical speculation.
Kapczynski Lens: Strategic Implication
Patent portfolio strategies for pharmaceutical clients in ASEAN should anticipate heightened scrutiny of secondary patent claims in jurisdictions that have internalized empirical anti-evergreening concerns. The Philippines is the current benchmark, but practitioner experience across the region suggests that Indonesia and Thailand are watching the evidence base closely.
Part II: The ASEAN Landscape: Country by Country
Armed with this theoretical framework, we turn to the practical landscape. The four jurisdictions examined here represent a spectrum of approaches, from Malaysia’s permissive flexibility to the Philippines’ strict gatekeeping that practitioners must navigate with precision.
At a Glance: The Regional Spectrum
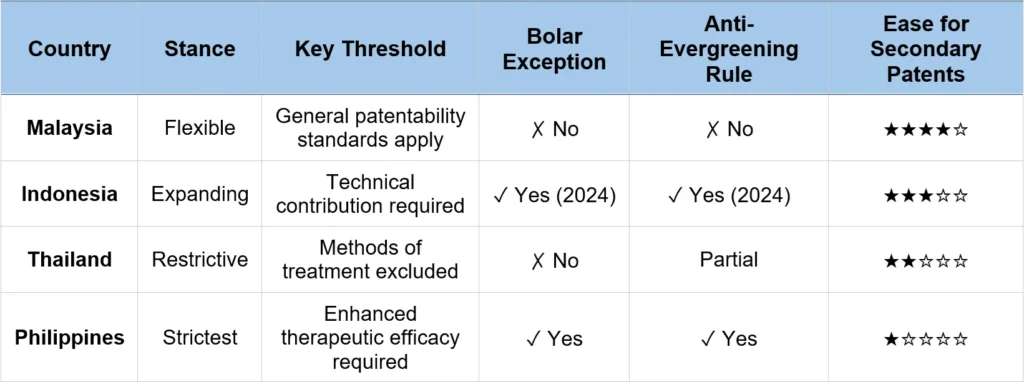

Malaysia: Permissive by Design and by Consequence
Malaysia’s Patents Act 1983 applies general patentability standards, novelty, inventive step, and industrial applicability without any pharmaceutical-specific carve-outs or anti-evergreening requirements. This makes Malaysia, from the perspective of a pharmaceutical innovator, the most accommodating jurisdiction in ASEAN for secondary patent prosecution.
What this means in practice: claims covering new salt forms, polymorphs, formulations, dosage regimens, and second medical uses are prosecutable on standard grounds. The patent examiner is not required to ask whether the claimed modification delivers enhanced therapeutic efficacy, only whether it meets general patentability criteria. Compound claims, formulation claims, Swiss-type use claims, and method of treatment claims (where allowable) are all within reach.
Applying Drahos’s framework: Malaysia’s permissive stance reflects a policy choice to prioritize pharmaceutical investment and innovation activity and the country’s ambition to be a regional pharmaceutical hub is well served by this approach. However, Drahos would note that the absence of pharmaceutical-specific patentability thresholds creates conditions in which low-quality secondary patents may be granted, potentially generating litigation uncertainty for both innovators and generic manufacturers.
Applying Burk & Lemley’s framework: The absence of policy levers calibrated to pharmaceutical innovation economics creates strategic uncertainty. In the absence of pharmaceutical-specific guidelines, prosecution outcomes depend heavily on examiner discretion, a variable that sophisticated patent counsel must account for through careful claim drafting and pre-filing strategy.
KASS Practice Insight: Malaysia
For pharmaceutical innovators, Malaysia represents a strong filing jurisdiction for building secondary patent portfolios. For generic manufacturers, the absence of formal anti-evergreening provisions means that pre-grant opposition and post-grant invalidation proceedings, supported by well-constructed prior art and obviousness arguments remain the primary defensive tools.
KASS advises early freedom-to-operate analysis before any generic entry decision in the Malaysian market.

Indonesia: The 2024 Transformation: A Reichman-Style Balance
Indonesia’s Law No. 65 of 2024 is the most significant development in ASEAN pharmaceutical patent law in a generation. To understand its implications, practitioners must grasp both what changed and what was specifically preserved.
Prior to 2024, Indonesia’s patent law imposed express restrictions on secondary pharmaceutical patents, limiting protection for new uses of known substances and certain variations of known products. The 2024 reform substantially relaxed these restrictions. Patents are now available for inventions such as second medical uses, provided they demonstrate a genuine technical contribution. The law’s illustrative example, Dapagliflozin, originally patented for Type 2 diabetes and subsequently patented for its use in treating chronic kidney disease signals that second medical use patents with documented clinical value will be examined on their merits rather than presumptively rejected.
"The most sophisticated pharmaceutical patent regimes are not those that most restrict or most permit, they are those that most precisely calibrate exclusivity to genuine contribution."
— Jerome Reichman, Calibrating IP Rights to Development Stage (2009)
Simultaneously, the 2024 law strengthened two critical public health safeguards. First, the expanded Bolar exemption now permits generic manufacturers to conduct testing, use, and production of patented medicines prior to patent expiry for the purpose of obtaining BPOM (the Indonesian Food and Drug Authority) regulatory approval, eliminating the lag time between patent expiry and generic market entry. Unlike the 2016 Patent Law, which limited such activities to the five years preceding patent expiration, the 2024 law does not impose any specific time limitation. Second, revised parallel import provisions allow patented medicines that have been placed on the market elsewhere in the world to be imported into Indonesia, helping to stabilize drug pricing.

Thailand: The Method Prohibition and Its Strategic Consequences
Thailand’s approach to secondary pharmaceutical patents is shaped by a categorical legal exclusion: methods of medical treatment and diagnosis are not patentable subject matter. This is not merely a procedural restriction, it reflects a fundamental policy determination that clinical medical decision-making should remain in the public domain, free from patent monopoly.
The practical consequence for secondary pharmaceutical patent strategy is significant. While patent protection is available for pharmaceutical compounds, compositions, and manufacturing processes, any claim that resembles a method of treating a medical condition faces categorical rejection. Thai patent authorities have historically subjected Swiss-type use claims, the industry’s preferred vehicle for second medical use protection to close scrutiny, frequently treating them as disguised method-of-treatment claims.
Applying Burk & Lemley’s framework: Thailand’s method exclusion represents a policy lever deliberately calibrated against pharmaceutical innovators’ preferred secondary patent claim type. The appropriate strategic response is not to challenge this policy choice, but to construct patent protection around it, emphasizing composition claims, formulation claims, and manufacturing process claims that do not implicate the method exclusion.
Applying Drahos’s framework: Thailand’s categorical approach reflects a social contract determination: that the public benefit of unrestricted clinical practice outweighs the innovation incentive created by method-of-treatment patents. Whether one agrees with this determination or not, practitioners must treat it as the stable background condition of Thai pharmaceutical patent strategy.
KASS Practice Insight: Thailand
In Thailand, pharmaceutical patent strategy requires careful claim architecture at the prosecution stage, not during litigation. Reliance on Swiss-type use claims as the primary form of secondary patent protection carries significant risk of rejection or invalidity.
KASS recommends a layered approach: compound claims at the earliest stage, supported by formulation and process claims that do not engage the method exclusion. Early FTO analysis is particularly critical given the interaction between the method exclusion and enforcement strategy.

Philippines: The Enhanced Efficacy Standard: Correa in Practice
The Philippines represents the most rigorous anti-evergreening jurisdiction in ASEAN. Its Intellectual Property Code requires that secondary pharmaceutical patent claims, covering modifications such as new salt forms, esters, polymorphs, metabolites, and particle-size changes, demonstrate enhanced therapeutic efficacy compared to the known substance. Without this clinical demonstration, the modification is treated as the same known substance and denied patent protection.
This is, in essence, the Correa framework enacted as positive law. The Filipino legislature and Intellectual Property Office have determined that the social contract of the patent system, exclusive rights in exchange for genuine contribution requires pharmaceutical secondary patents to clear a materially higher bar than non-pharmaceutical inventions, because the stakes (patient access to affordable medicines) are correspondingly higher.
"The Philippine framework correctly identifies that patent law should not be indifferent to what kind of improvement is being claimed and in pharmaceutical secondary patents, only clinical improvement justifies an extension of exclusivity."
— Carlos Correa, Public Health and Intellectual Property Rights (2004)
The practical implications for prosecution are significant. A polymorph of a known pharmaceutical compound must be accompanied by evidence, typically clinical or pharmacological data, demonstrating that it provides materially better therapeutic outcomes than the known form. A new salt must show improved bioavailability with clinical consequence. A new use claim must identify a therapeutic indication that represents a genuine advancement in treatment, not merely a label extension.
Applying Kapczynski’s framework: The Philippines’ strict stance is empirically grounded: the evidence base on pharmaceutical evergreening, to which scholars like Kapczynski have contributed, directly supports the legislative choice to require demonstrated clinical advantage. For innovators, this creates a high evidentiary bar at prosecution but it also means that patents granted under this standard are more likely to survive post-grant challenge, because they represent genuinely defensible inventions.
KASS Practice Insight: Philippines
Philippine pharmaceutical patent prosecution requires early investment in clinical data development. Patent applications that rely solely on in vitro evidence of improved stability or solubility, without demonstrated therapeutic consequence, face significant rejection risk.
KASS’s Philippines team works closely with clients’ regulatory and clinical affairs functions to ensure that the evidentiary record supporting a secondary patent application is constructed before, not after, the patent application is filed.
Part III: Strategic Synthesis: What Practitioners Need to Know
The four country profiles above reveal a regional landscape that does not follow a single coherent logic. Practitioners who apply uniform patent prosecution strategies across ASEAN will encounter systematic failures, not because of procedural errors, but because the underlying policy frameworks are genuinely different in ways that require different substantive approaches.
For Pharmaceutical Innovators
The central strategic imperative is jurisdictional differentiation. A secondary patent portfolio built for Malaysia where general patentability principles apply will not translate automatically to the Philippines, where enhanced therapeutic efficacy is required. Prosecution strategies, claim architectures, and supporting evidence packages must be tailored to each jurisdiction from the outset.
Indonesia’s 2024 reforms deserve particular attention. Pharmaceutical innovators who have not reviewed their secondary patent portfolios in light of Law No. 65 of 2024 are operating with outdated intelligence. The expansion of protectable subject matter, particularly second medical uses represents a material change to the Indonesian pharmaceutical patent landscape that should trigger a systematic portfolio review.
Regional Filing Strategy Recommendation
Prioritize Malaysian and post-2024 Indonesian filings for broad secondary patent coverage. Build Swiss-type use claim strategies for Indonesia carefully, with attention to the genuine technical contribution requirement. For Thailand, invest prosecution resources in composition and formulation claims rather than use claims. For the Philippines, ensure that clinical data packages are patent-prosecution-ready before filing and budget for data-generation timelines accordingly.
For Generic Manufacturers
The Philippine framework offers the most favorable defensive environment in ASEAN, secondary patents that clear the enhanced efficacy bar are genuinely strong, but far fewer secondary patents will reach that bar. Pre-launch freedom-to-operate analysis should carefully assess whether secondary patents in the Philippine portfolio reflect genuine therapeutic advances or represent vulnerable claims.
Indonesia’s expanded Bolar exemption is a material operational advantage for generic manufacturers: it now permits parallel development of generic versions during the innovator patent term, compressing the time to generic market entry after patent expiry. Generic manufacturers who are not yet taking full advantage of the expanded Indonesian Bolar exemption are leaving competitive lead time on the table.
Thailand’s method exclusion creates natural gaps in pharmaceutical patent protection that generic manufacturers and their freedom-to-operate analysts should map systematically against innovator patent portfolios before making entry decisions.
The Practitioner's Overarching Principle
"The global patent system is not a single system. It is a patchwork of national social contracts, each calibrated to different development imperatives, different institutional capacities, and different public health priorities. The practitioner who treats it as uniform operates at systematic risk."
— Peter Drahos, A Philosophy of Intellectual Property (1996)
Drahos’s observation resonates with particular force in ASEAN pharmaceutical patent practice. The four jurisdictions examined here are not merely administrative variants of a common regional framework. They represent fundamentally different legislative choices about the relationship between pharmaceutical innovation, public health access, and the social contract of patent exclusivity.
Understanding these differences at the level of the theoretical frameworks that animate them, not merely at the level of procedural rules is what distinguishes sophisticated pharmaceutical patent practice from routine prosecution. It is the difference between a strategy built for ASEAN and a strategy that merely happens to file in ASEAN.
Conclusion: The Productive Tension at the Heart of Secondary Patents
Secondary pharmaceutical patents sit at the intersection of two legitimate imperatives that cannot be fully reconciled: the imperative to protect genuine innovation and thereby sustain the R&D investment that produces new medicines, and the imperative to ensure that medicines reach the patients who need them at prices that do not exclude entire populations.
The five top thinkers whose frameworks animate this analysis do not all answer the resulting question in the same way. Drahos and Correa are skeptical of secondary patent regimes that do not demand genuine therapeutic contribution. Reichman argues for calibrated flexibility that serves both innovation and access. Burk and Lemley urge sectoral precision in the application of patentability standards. Kapczynski grounds the debate in empirical evidence about pharmaceutical patenting behavior.
What they share is a recognition that this is a question about the design of social institutions and that the answer differs legitimately across jurisdictions at different stages of development, with different public health burdens, and different domestic pharmaceutical industries.
For practitioners, this means that the most important skill in ASEAN pharmaceutical patent practice is not mastery of any single jurisdiction’s rules, but the capacity to read the theoretical orientation of each jurisdiction’s framework and to construct strategies that are aligned with, not merely compliant with, those orientations.
KASS International has built its regional IP practice on exactly this capacity. Our teams in Malaysia, Indonesia, Thailand, and the Philippines work within a common analytical framework while bringing deep local knowledge of how each jurisdiction’s rules are applied in practice. For pharmaceutical patent strategy in Southeast Asia, that combination, regional coherence and local depth is not optional. It is the practice standard.
About KASS International
KASS International is a leading regional intellectual property firm headquartered in Kuala Lumpur, with offices across Southeast Asia including Indonesia, Vietnam, Thailand, Singapore, Philippines, and Myanmar. Ranked in the IAM Patent 1000 2026 -> Gold tier in Malaysia, with recognition across Indonesia, Vietnam, and Thailand, KASS combines regional breadth with deep country-level expertise.
Our pharmaceutical patent practice advises multinational innovators, regional generic manufacturers, and research institutions on patent prosecution, portfolio strategy, freedom-to-operate analysis, and enforcement across all ASEAN jurisdictions.
© KASS International. All rights reserved. This article is intended for practitioner information purposes and does not constitute legal advice.